
Suicide Assessment | Part 2 Gathering Information: Ask/Listen/Clarify

In Part One of this series on Suicide Assessment, I introduced a Framework to Guide Assessment based on the Four Core Principles used by 988 centers nationwide. Here, in Part 2, I will begin to explore how, in conversations with your client, you can begin to gather the information needed for your full assessment, focusing on how to ASK about suicide, LISTEN to your client’s story, and CLARIFY missing pieces of your assessment.
Knowing about risk and protective factors for suicide, recognizing warning signs of immediate danger, and understanding the Four Core Principles of Assessment are helpful foundational steps to developing a confident approach to the assessment of suicide risk. Yet even with this knowledge, engaging clients in an open conversation about their thoughts of suicide - while you gather details essential to understanding their risk - presents its own challenges.
ASK
Talking to clients about suicide is stressful, even for the most experienced clinician - even if it's something you do all the time. I have worked in the field of suicide prevention for over 25 years and yet I still experience a moment’s pause before the word suicide comes out of my mouth. It’s just not easy. But whenever you have any concerns about suicide, you must ask about it, and you must ask about it directly:
Are you thinking of suicide?
Are you thinking of killing yourself?
Practice saying these questions until you can say them without hesitation. Use the word “suicide” - say it out loud when alone or practice these questions with colleagues - anyway that helps increase your comfort. Avoid softer language: you don’t want to ask, “Are you thinking of harming yourself?” (unless you intend to ease into asking directly about suicide as a follow-up question). Asking alone about “harming yourself” can be misleading - they may say no - they are not actually thinking of harming themselves they are considering ending their life, and these are two very different things.
During an intake with a client it is likely a bit easier to ask directly about suicide - given that you are gathering information and it is expected that you will have a range of questions about an individual's history and current needs. Many clinicians will use suicide screeners - such as the ASQ5 or the C-SSRS Screener (more on use of assessment scales in future post) - and each of these will address suicide directly - but I tend to find that most clinicians in private practice do not use screening tools when first meeting with client or in their practice at all - so it is always good to know ahead what you will actually ask. As a general intake question, you can ask directly about suicide as follows:
Have you had any thoughts of suicide in the last few months/days, including today?
You want to know about lifetime risk - but you also want to know about today, right now. The reason not to do just one or the other, and to also phrase the question to include recent months/days, is that many people may feel safer acknowledging previous thoughts or behaviors rather than discussing the more immediate situation. Other questions you can ask include:
Have you ever had thoughts of suicide/killing yourself?
Have you ever attempted to kill yourself?
Have you EVER taken any action to harm yourself, including today? [this last clarification can be especially relevant in remote sessions where it can be unclear if a client has already ingested pills or undertaken any action to harm themselves].
If your client acknowledges a suicide attempt history, be sure to ask about details of the attempt. It is important to begin to understand the lethality and their feelings on the fact of their survival. It can also be useful to know about interrupted or aborted attempts that a client may not consider reporting.
During ongoing work with clients, talking about suicide can be much more challenging. You may have been working with a client for some time - even someone with no history of suicidal thoughts - where the need to address the issue arises. Here, it's good to remember that, as difficult as it may be for you to talk about suicide it's likely significantly harder for your client. Many people are reluctant to share thoughts of suicide and there are many valid reasons why - they may fear your response, being judged, or that you will no longer want to work with them. They may fear needing to involve family or friends. Many often fear that therapists will jump to hospitalization and be unable to tolerate the conversation. They also may have had bad experiences in the past when talking about suicide. So remember - for some people, this may be the first time they have been able to express their thoughts of suicide out loud - and your job is to provide a safe, non-judgmental, open space for them to explore these thoughts and hopefully work with you to remain safe after they leave.
Given that clients could be reluctant to bring up the issue of suicide, it is essential that you do what we call - listening for invitations - where a client offers an opening to begin the conversation. Invitations to talk about suicide come in many forms. Of course, there are some clearer indications reviewed in risk factors - maybe they have had a decreased mood or seem hopeless. But not everyone with thoughts of suicide will look as you may expect them to look - invitations, therefore could just sound like statements such as:
“It's all too much for me, I can’t go on like this.”
“All of my problems will end soon.”
“No one can do anything to help me now.”
”I am a burden to everyone.”
These could well be invitations to you to ask them about how they are feeling - and whether they are having thoughts of suicide.
When you say your problems will end soon, what do you mean by that?
Do you mean you are having thoughts of killing yourself?
Be mindful of phrasing and avoid negative statements
You’re NOT thinking of killing yourself are you?
which as you can imagine sends a clear message that this is not what you want to hear.
LISTEN
Then there is the moment when your client replies
Yes, I am thinking of suicide.
Acknowledge what your client has said and ask
Can you tell me more about that?
Let your client tell their story. Let them describe their thoughts of suicide - are they fleeting? Intrusive? Distressing? How does it feel to have these thoughts? For some people, thoughts of suicide occur all the time - they carry them like a safety blanket - "Oh it's ok I can handle this - if anything goes wrong I can just kill myself" - but they have never really had any active intent (this is of course no no less important to address in terms of focusing on safety planning - but it is likely quite different from someone who has intrusive thoughts that scare them) - what does this person do when these thoughts arise?
It can be useful to ask your client
What stops you from killing yourself?
In listening to their story, you are gathering information for your assessment. Listen for elements that can inform both your assessment of their safety as well as the development of a safety plan for later.
When listening to a suicide narrative, you will likely hear many reasons for dying - but there will likely also be many things mentioned that are reasons for living. As strong as someone may feel about dying, something has kept them alive to this point and some level of internal ambivalence is likely why they are talking to you today. Your goal is to tip the balance to the side that wants to live.
A Note on Ambivalence
Ambivalence in the context of suicide refers to the simultaneous experience of conflicting thoughts and feelings about living and dying. It is a very complex and very common occurrence for those who are contemplating suicide and understanding this concept is extremely important for mental health professionals.
Ambivalence often involves a deep struggle between the desire to escape pain and the desire to live. A person may feel hopeless and despairing, yet also experience moments of connection, purpose, or love. This internal conflict is not only distressing but also difficult to express, often due to shame or fear of judgment. Ambivalence is also not static—it can change over time. A person’s emotions may shift based on external circumstances, the presence of supportive relationships, or changes in their mental health. During times of crisis or acute distress, these conflicting emotions can become more pronounced, driven by stressors like relationship problems, financial issues, or mental health crises.
Ambivalence can be seen most acutely when someone walks into your office and tells you they are having thoughts of suicide. No one likely forced this person to come and tell you this - and so while there may be one part of your client that wants to die, there is another part that is right in front of you and asking you to help them live.
Your client’s AMBIVALENCE is your OPPORTUNITY
CLARIFY
As you listen to your clients story and gather information, it is important to remember the four core principles of your assessment and clarify any missing pieces. Ask yourself:
Is there evidence of intent, and capability?
What buffers (safety measures) are in place?
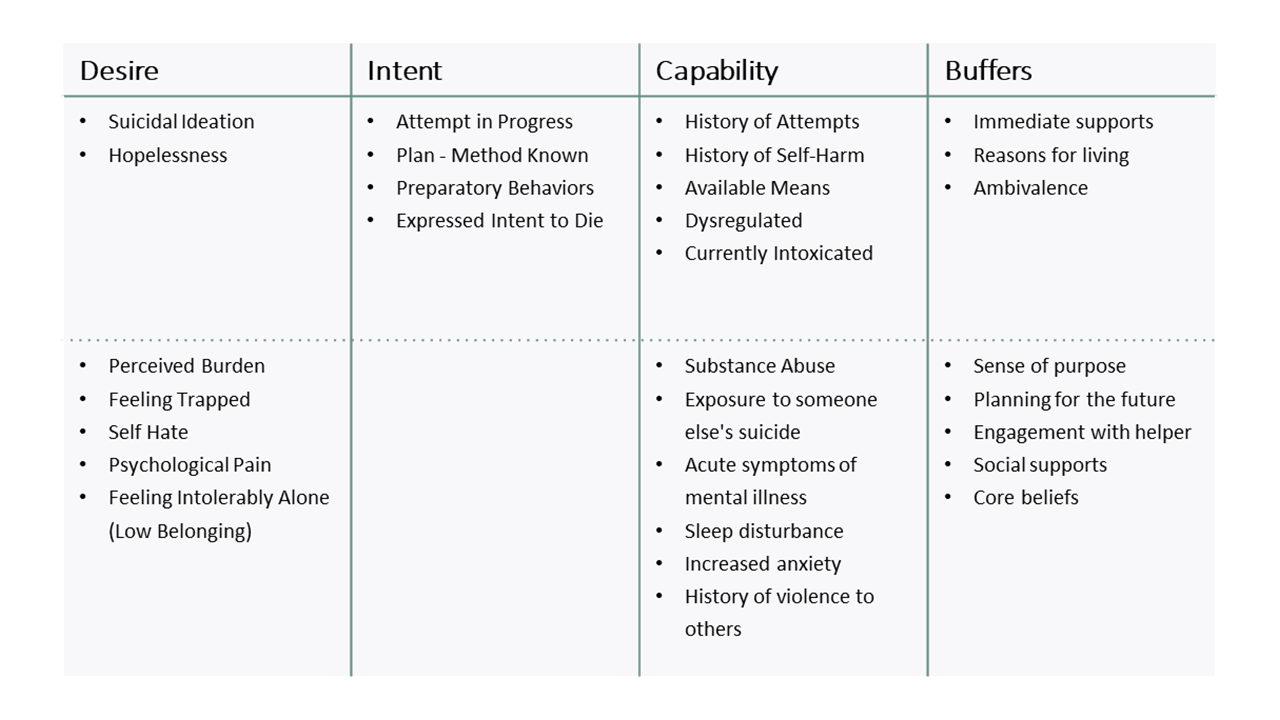
Clarify Intent: What else do I need to know about my client’s intent to act on their thoughts of suicide? Did they clearly express an intent to die? Have I heard all I need to know about any method that has been considered or plans that have been made?
Clarify Capability: What do I know about their history of attempts or self-harm,? Do they seem dysregulated or intoxicated? Are they sleeping? In particular, what do I know about their access to lethal means? Does this person own a gun?
Clarify Buffers: What do I know about my client’s support system? Do they live alone? Who do they talk to about their thoughts of suicide? Have I heard them express any reasons for living?
Once you have gathered what you need, it will be time to formulate the degree of risk you believe to be present and, based on that, begin to plan how you will help your client stay safe.
In my final post on assessment, I will explore the process of Formulating Risk and how we use this to PLAN with our clients for safety.
ASK about suicide
LISTEN to your clients thoughts of suicide
CLARIFY missing pieces (intent, capabilty, buffers)
PLAN for safety (risk formulation and intervention)
Would you like more in-depth training in Suicide Safety?

Join the newsletter to receive FREE access to a chapter of the online course: