
Suicide Assessment | Part 1 A Framework to Guide Assessment

Most training on suicide prevention and intervention typically begins with foundational topics: suicide statistics, a thorough review of factors influencing risk, the impact of professional biases, and an overview of available screening tools and standardized scales. Only then would the focus shift to assessment and intervention strategies. In this blog series, however, the information is structured differently—prioritizing practical strategies for immediate application in clinical practice, with foundational information introduced later to reinforce and build on these skills.
Guidance provided here on Suicide Assessment emphasizes a conceptual approach, designed to prepare clinicians to respond effectively when clients share suicidal thoughts or when risk is suspected. The focus is on assessing "safety for now" and building confidence in forming a clear plan of action with clients to maintain that safety. Given the amount of information, the series is organized into three parts:
Part One will provide a brief overview of the various factors that contribute to increased suicide risk. Rather than delving into the underlying reasons for each factor’s impact, an emphasis will be placed on introducing a Framework to Guide Assessment based on the Four Core Principles of Suicide Assessment used by 988 centers nationwide.
Part Two will discuss Gathering Information, focusing on how to ASK about suicide, LISTEN to our client’s story, and use this framework to CLARIFY missing pieces of our assessment.
Part Three will explore the process of Formulating Risk and how we use this to PLAN with our clients for safety.
Overall, I hope this series provides clinicians with an approach to managing safety using a structured yet flexible approach to guide the assessment process.
What Places People at Suicide Risk?
While there is no single cause for suicide, certain factors are known to increase the risk of an attempt, making an understanding of these elements essential to effective suicide care. Any discussion on suicide risk typically begins with a focus on the range of contributing factors. This includes examining established risk and protective factors, recognizing warning signs of immediate danger, and identifying person-specific factors that may contribute to suicidal thoughts.
RISK FACTORS: Risk factors for suicide refer to any factors that increase the likelihood that an individual will consider, attempt, or die by suicide. The CDC groups these into personal, relationship, community, and societal risk factors (see below).
NOTE: The CDC groups protective factors into the same four categories - many of these are direct counters to the presented risk factors and can be viewed here.
-
Previous suicide attempt
History of depression and other mental illnesses
Serious illness such as chronic pain
Job/financial problems or loss
Impulsive or aggressive tendencies
Substance misuse
Current/history of adverse childhood experiences
Violence victimization and/or perpetration
Sense of hopelessness
-
Bullying
High conflict or violent relationships
Family/loved one’s history of suicide
Loss of relationships
Social isolation
-
Lack of access to healthcare
Suicide cluster in the community
Stress of acculturation
Community violence
Historical trauma
Discrimination
-
Stigma with both help seeking and mental illness
Easy access to lethal means
Unsafe media portrayals of suicideItem description
WARNING SIGNS: Warning Signs refer to indications of more immediate risk. Risk factors and warning signs for suicide have been compared to the way in which we identify the warning signs for a heart attack. Risk factors for heart disease can include smoking, obesity, and high cholesterol – these factors increase the likelihood that someone could suffer a heart attack at some point in their lives. Warning signs, however, such as chest pain, shortness of breath, and nausea, indicate that someone may be having a heart attack right now.
-
Indications of more immediate risk
Becoming isolated or withdrawing
Talking about feeling trapped or in unbearable pain
Increased substance use
Looking for a way to access lethal means
Increased anger or rage or extreme mood swings
Expressing hopelessness, feeling trapped, or a burden
Sleeping too little or too much
Talking or posting about wanting to die
Making plans for suicide
DRIVERS: Suicide Drivers* are those factors that may elevate a person’s risk at a specific moment in time. They are person-specific, meaning they refer to the unique elements directly "driving" an individual toward thoughts of suicide. These factors often relate to relationship issues, intense suffering or anxiety, vocational concerns, or feelings of low self-esteem and self-hatred.
Suicide drivers can often identified by asking yourself….
What is happening in my client’s life right now that is moving them towards thoughts of suicide?
Assessment Framework: Four Core Principles
A notable aspect of reviewing the factors that place people at risk for suicide is the sheer number of risk factors, warning signs, and suicide drivers to consider in the assessment process. For clinicians, the question becomes
What am I supposed to do with all this? Almost everything a person experiences could place them at risk for suicide.
One helpful way to look at all these risk factors and the assessment itself is through the lens of the 988 Suicide & Crisis Lifeline Safety Assessment Model.** This model includes, in its central assessment stage, what are referred to as the Lifeline Four Core Principles of Suicide Assessment which serve to group the wide range of available risk factors into a more useful and useable framework through which to view the assessment process.
These principles, which draw from the central concepts of the Interpersonal-Psychological Theory of Suicide (IPTS) developed by Thomas Joiner, propose that the combination of suicidal desire with intent and an acquired capability is associated with heightened risk for suicide.
Specifically, Joiner's theory proposes that a combination of feeling like a burden to others and experiencing social alienation can lead to a DESIRE to die which in turn can progress to suicide INTENT, where the individual makes plans, or takes preparatory actions. Joiner argues, however, that individuals will not act on this desire unless they overcome the instinctive drive for self-preservation—the innate fear of death. He refers to this as “acquiring the CAPABILITY” to die, which develops through repeated exposure to painful or provocative experiences, leading to habituation. Examples include previous suicide attempts, non-suicidal self-injury (NSSI), childhood trauma, combat exposure, physical pain, and more. Joiner’s theory was groundbreaking in explaining the process of developing suicidal ideation and why many of those who experience suicidal thoughts do not attempt suicide—they haven’t acquired the capability to do so.
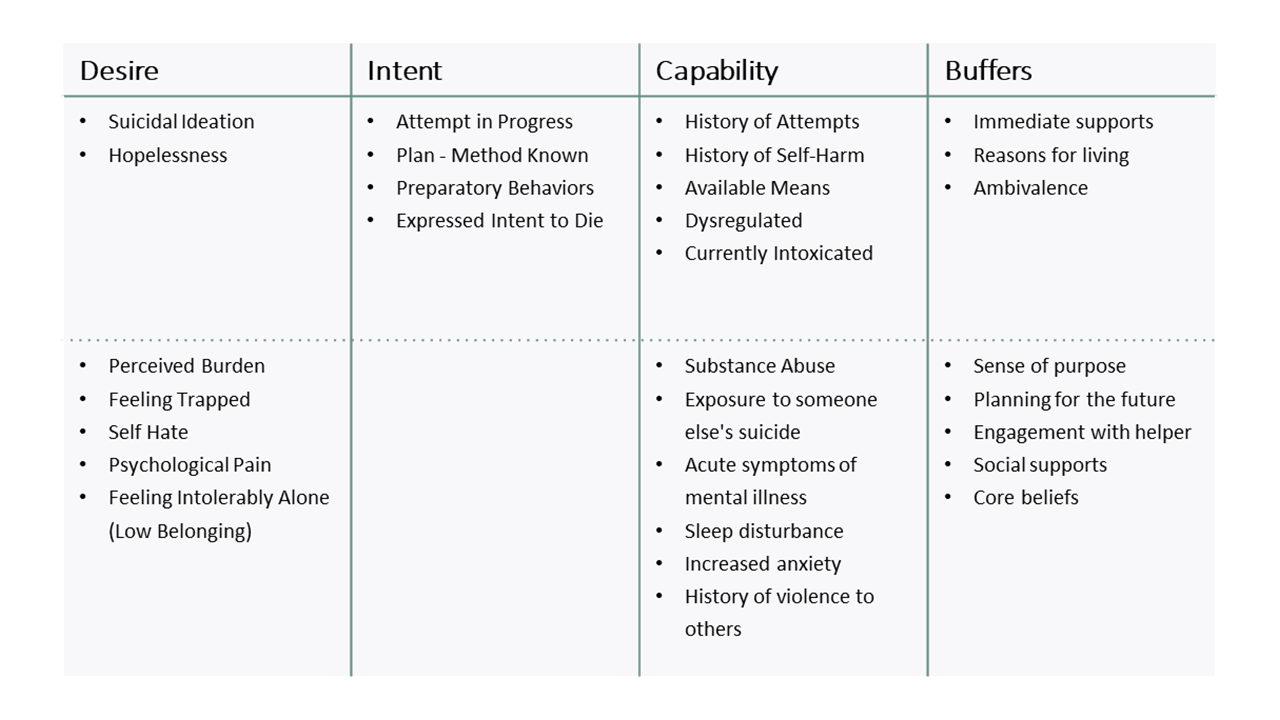
The Lifeline Four Core Principles focus on these areas - Desire, Intent, and Capability, with Buffers added to also consider any elements that could serve to mitigate that risk. The table below outlines how many of the risk factors/warning signs mentioned above are grouped under these core principles. ***
When we undertake an assessment guided by these Four Core Principles we focus on:
1. SUICIDE DESIRE (“I want to kill myself”)
Desire refers to the individual’s acknowledgment of suicidal thoughts and possible feelings of hopelessness, worthlessness, intolerable loneliness, or feeling like a burden to others. Your client may explicitly state, "I want to die," “I want to kill myself” “I’m thinking of suicide” but even if they don’t, listen for statements that reflect a strong desire for suicide.
2. SUICIDE INTENT (“I am going to kill myself”)
Intent reflects the likelihood of taking action. This could include the presence of a specific plan or engagement in preparatory behaviors. Your client may explicitly express their intent to act on the suicidal thoughts they have or, in some cases, an attempt may be in progress (this is especially relevant in remote sessions where it can be unclear if a client has already ingested pills or undertaken any action to harm themselves).
3. SUICIDE CAPABILITY (“I am able to kill myself”)
Capability refers to whether a person has access to lethal means or a history of any form of self-harm, particularly past suicide attempts, that may contribute to a reduced fear of death. We know that the most significant risk factor for future attempts is a past suicide attempt so it is always important that you explore this fully with your client. Regardless of attempt history, I always discuss access to lethal means, especially firearms, and address this as a priority.
4. SUICIDE BUFFERS (“I have reasons not to kill myself”)
Finally, buffers are protective factors that mitigate risk. These include immediate support systems, relationships, or the individual’s ambivalence toward dying (to be discussed in Part 2). It is important here not to completely rely on buffers to mitigate your client’s risk. If your client demonstrates desire, intent, and capability, buffers may not be sufficient to reduce risk.
Application to Practice
How does grouping factors this way help with my assessment?
In clinical practice, when assessing suicide risk, this framework directs attention to four key elements:
What do I know about my client’s DESIRE, INTENT, CAPABILITY, and BUFFERS?
This focus is what I find most useful. In potentially stressful moments, when a client shares thoughts of suicide, instead of trying to recall every possible risk factor or follow a lengthy screening tool, I rely on this framework to guide my assessment.
When a client expresses thoughts of suicide (DESIRE), I immediately consider their INTENT and CAPABILITY. To better understand the intensity of these thoughts, I often ask them to rate their DESIRE to die on a scale of 1 to 10. A rating of 7 or 8, for example, indicates a strong desire to die.
Next, I consider INTENT. Have they developed any specific plans? Using the same scale, I may ask about their intent to act on suicidal thoughts. A similar rating of a 7 or 8 will alert me to a heightened risk. A lower rating (e.g., a 3) can provide some reassurance that while they are having thoughts of suicide, their intent to act is not strong.
Regardless of the ratings for desire and intent, when a client shares thoughts of suicide, I always assess CAPABILITY. This includes considering any history of attempts or self-harm and discussing access to means, both of which are essential to understanding risk and determining an appropriate response.
While asking clients to rate the intensity of their experience is not a standard part of this framework, it can be a valuable tool for reflection. It allows clients to pause and consider the severity of their suicidal thoughts while providing clinicians with additional insight into intent. The ratings themselves do not determine the course of action; instead, they guide the conversation, creating an opportunity to demonstrate that open discussions about suicidal thoughts are safe and encouraged, particularly when intent and capability are not an immediate concern. The reality is that many individuals experience suicidal thoughts without having any intent to act. Introducing the conversation in this way helps to normalize discussions about suicide and allows clients to express their fears openly.
In the next post I will explore how, in conversations with your client, you can begin to gather the information needed for your full assessment, focusing on how to ASK about suicide, LISTEN to your client’s story, and use the framework outlined to CLARIFY any gaps in your assessment data.
* The concept of suicide drivers is primarily outlined in the Collaborative Assessment and Management of Suicidality (CAMS) framework developed by David Jobes. See below for additional reading.
** The Lifeline Safety Assessment Model is not reviewed here for simplicity but will be referred to later in the series.
*** You will notice the division of elements above and below the dotted line on this chart. These elements were grouped this way to further focus clinicians on those factors essential for assessment (above the line) and those that, while also important and relevant, may be more client or situation-specific. Meaning, those elements above the line are prioritized and essential to know in your assessment of risk.
If you have questions or comments about the model, I have added a comments option at the bottom of this page.
Further Reading
Jobes, D. A. (2023). Managing Suicidal Risk: A Collaborative Approach (3rd ed.). New York, NY: Guilford Press
Joiner, T. E. (2005). Why people die by suicide. Cambridge, MA: Harvard University Press
Joiner, T. E., Kalafat, J., Draper, J., Stokes, H., Knudson, M., Berman, A. L., & McKeon, R. (2007). Establishing standards for the assessment of suicide risk among callers to the National Suicide Prevention Lifeline. Suicide and Life-Threatening Behavior, 37, 353-365.
Would you like more in-depth training in Suicide Safety?

Join the newsletter to receive FREE access to a chapter of the online course: